
If you're looking for help managing medications for someone with dementia, you're probably here because the situation has shifted recently. A parent who used to handle their own prescriptions is missing doses, or doubling them, or insisting they already took something they didn't. A spouse with a recent diagnosis is in the awkward middle ground where they're capable but no longer reliable. You're trying to figure out how to keep them safe without taking over more than you need to.
This guide is for that situation. What follows isn't medical advice, and it isn't a prescription routine that fits every family. It's a practical look at how medication management actually works when the person taking the medication can't fully manage it themselves, and what tools, strategies, and conversations help.
A note on what this article covers and doesn't: this is about coordination, tools, and caregiver workflows. Specific clinical questions about which medications to take, doses, side effects, or interactions belong with your loved one's doctor or pharmacist. The goal here is the management problem, not the medical one.
Why dementia changes medication management
In a typical adult life, medication management is a personal responsibility. You take your pills, you remember whether you took them, and if there's a question you can answer it yourself. Dementia breaks this whole loop.
Three specific things go wrong, in roughly this order as the condition progresses:
Memory becomes unreliable. Early on, the person may genuinely intend to take their medications and believe they have, even when they haven't. They may take a dose, forget within minutes that they did, and take it again. The most dangerous version of this isn't the missed dose; it's the duplicated dose, especially with medications where overdose carries real risk.
Self-reporting becomes unreliable. When you ask "did you take your morning pills?" the answer you get may not match reality. This isn't dishonesty. The person believes what they're telling you. The internal record-keeping that lets a healthy adult say "yes, I took it about an hour ago" simply isn't working. This makes verification by anyone other than the person themselves essential.
Recognition fades. As dementia progresses, the person may stop recognizing their own medications, stop understanding why they're supposed to take them, and eventually need full hand-over-hand assistance. The transition from "I'm reminding Mom to take her pills" to "I'm physically administering Mom's pills" happens gradually, and the right tools and routines for the early stage aren't the same as the right ones for the later stages.
Recognizing where in this arc your loved one is matters, because the right approach changes as the disease progresses. What works at the early stage will fail at the middle stage, and middle-stage strategies don't address late-stage realities. Plan for the current stage but expect to revisit the system every few months.
The basics that still apply
Before getting into dementia-specific strategies, a few principles from general medication management still hold, just with more weight behind them.
A consistent daily routine helps more than anything else. The Alzheimer's Association recommends developing a routine around medication times: tying doses to meals or bedtime, doing them in the same place at the same time each day. For someone whose memory is unreliable for facts but often still strong for habits, embedding medication into the rhythm of the day is more reliable than asking them to remember a clock time.
A pill organizer is non-negotiable. Weekly pill organizers with separate compartments for each day (and ideally each time of day) provide visual confirmation of what was taken and what wasn't. The person can see "Monday is empty, Tuesday is full, today is Tuesday morning" without remembering anything. For caregivers who aren't present, a quick photo of the organizer answers the question of whether doses were taken without requiring the person to remember.
A pill organizer's limit is that it tells you a compartment is empty but not who emptied it or when. For a single caregiver in the home, that's enough. For situations where multiple family members are involved, where the patient may have emptied a compartment without taking the contents, or where you need a record of what was given for the doctor's visit next week, you'll eventually need something more. A pill organizer answers "was the dose taken." A medication tracking app answers "was it actually administered, by whom, and at what time," which becomes the more important question as the situation gets more complex.
Keep an updated medication list. Every dementia caregiver should have an accurate, current list of every medication the person takes: name, dose, time, prescribing doctor, reason. This list lives somewhere reliable (a refrigerator door, a binder, a phone app) so that when an emergency happens, anyone can answer the question of what the person takes. Update it every time anything changes.
Coordinate with the pharmacy. Most pharmacies will arrange synchronized refills so all medications are due at the same time each month, and many offer blister-pack pre-sorting where each dose is sealed in its own labeled compartment. Both of these reduce caregiver burden significantly. Ask the pharmacist what services they offer for caregivers managing someone else's medications.
These basics are the foundation. Everything below builds on them.
Strategies specific to dementia
Once the general system is in place, dementia introduces problems that ordinary medication management doesn't have to solve. Each of these is worth thinking through for your specific situation.
Lock up the medications. This is the single most important safety step, and the Alzheimer's Association names it explicitly: keep medications in a locked drawer or cabinet to prevent accidental overdose. The person with dementia may take a dose, forget, see the bottle, and take another. Or take medication that isn't theirs, thinking it belongs to them. A locked cabinet with a single accessible weekly organizer (refilled by the caregiver) is the structure that prevents both these failure modes.
Verify rather than ask. Asking "did you take your pills?" gets you an answer the person believes is true but may not be. Instead, verify directly: look at the pill organizer, check the blister pack, check the medication tracking app. If the verification shows the dose was taken, fine. If it shows the dose wasn't taken, you know without putting the person on the spot. This protects their dignity while protecting their safety.
Simplify whenever possible. Talk with the prescribing doctor and pharmacist about whether the medication schedule can be simplified. Sometimes a medication that's taken three times a day has an extended-release version that's taken once. Sometimes two medications can be combined into a single pill. Sometimes a medication that's been on the list for years is no longer necessary. A simpler regimen is easier to manage and easier for the person to participate in to whatever extent they still can.
Match the cue to the dose. Pair specific medications with specific daily events. Morning pills go with breakfast coffee, in the same room, every day. Evening pills go after dinner cleanup, before the favorite TV show. The pairing creates a context cue that aids habitual memory even when episodic memory is failing. Avoid scheduling doses at times that aren't anchored to anything else.
Use simple, clear instructions. When prompting someone with dementia to take medication, the Alzheimer's Association recommends simple language and clear instructions. "Here are your morning pills. Let's take them with your coffee." Not "Did you remember your medications? Don't forget to grab them before breakfast." The first lands. The second creates pressure without giving direction.
Plan for resistance. At some point, many people with dementia resist medication, sometimes because they don't recognize the pills, sometimes because the act of being told what to do feels controlling, sometimes for reasons that aren't legible to anyone. If this starts happening, talk with the doctor about alternatives: liquid forms that can be mixed with food, transdermal patches for some medications, or tablets that can be crushed (only some can; ask the pharmacist first). The goal is to make taking the medication feel like a small, normal part of the day rather than a confrontation.
Tools and reminders that work
The "medication reminders" part of this article is the part most people are searching for, but it's worth being honest: no app or device fully solves dementia-related medication management on its own. The tools work as part of a system that includes a caregiver, a routine, and clear visual structure. For families earlier in the progression who are still evaluating the general landscape of reminder systems for an elderly parent, medication reminders for the elderly covers how each category compares before dementia-specific considerations take over.
That said, several categories of tools earn their place.
Pill organizers with alarms. Electronic pill organizers with built-in alarms (devices like MedReady, Hero, Livi) dispense the correct dose at the correct time and beep until the dose is taken. The advantage over a passive pill organizer is the audible cue. The disadvantage is they cost more, require setup and maintenance, and can become a source of confusion in late-stage dementia if the person doesn't understand why the device is beeping.
Smartphone or tablet apps. A phone-based medication reminder app works well for early-stage dementia when the person still uses their phone reliably. As the condition progresses, app-based reminders become less effective because the person stops responding to or recognizing the reminder. At that point, the value of the app shifts from prompting the patient to coordinating the caregivers: tracking what was given, by whom, and when, across multiple family members.
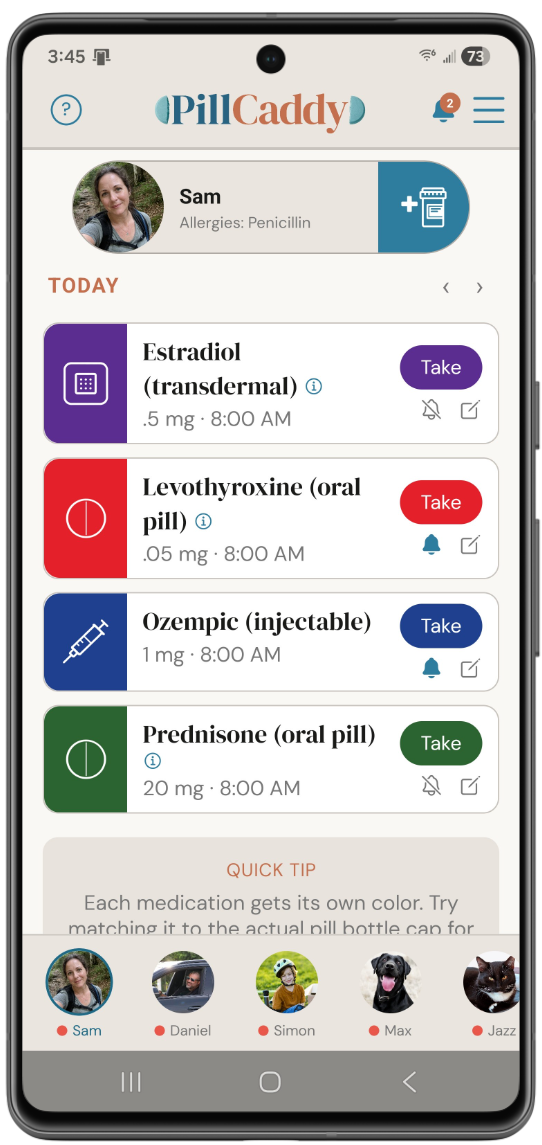
Shared family tracking. This is often where the real value lives for dementia caregivers. When the medication is being administered (not just self-managed by the patient), the question isn't "did Mom take her pills?" It's "did anyone give Mom her pills?" If two siblings and a home health aide are all involved in care, you need a shared record that updates in real time. PillCaddy is built for exactly this: anyone with permission can mark a dose as given, and everyone else immediately knows. The texting-back-and-forth that consumes so much of a caregiver's energy goes away.
Pharmacy blister packs. Many pharmacies will pre-sort medications into weekly or monthly blister packs where each dose is in its own sealed, labeled compartment. For a caregiver managing someone else's medications, this is one of the highest-leverage simplifications available: no weekly pill-sorting, immediate visual confirmation of what was taken, and a structure that's hard to misuse.
Whiteboards and analog cues. For some patients, especially those who are still home alone for parts of the day, a large whiteboard in the kitchen with the day's medications listed and a place to check off each one provides a visible structure that doesn't depend on technology. This works best paired with a daily phone call from a caregiver to verify.
The right tool depends on your loved one's stage of dementia, your family's coordination needs, and what fits the existing daily rhythm. Most caregivers end up using a combination: a pill organizer for structure, a tracking app for caregiver coordination, and direct administration for whatever the person can't manage themselves.
When multiple family members are involved
Many dementia care situations involve more than one caregiver: spouses, adult children, grandchildren, professional in-home aides, sometimes neighbors who check in. The medication problem in these households isn't just "did the patient take their pills"; it's "do we, as a group, know what was given and when."
The classic failure mode is the duplicated dose. Sister visits in the morning and gives the morning pills. Brother stops by at lunch, asks Mom if she took her pills, hears "I don't think so" (which may not be true), and gives them again. The patient ends up with two doses of everything, and depending on the medications, that can be anywhere from inconvenient to dangerous.
The fix is a shared record that everyone updates in real time and can check before administering anything. Whether that's a paper logbook on the kitchen counter, a group text thread, or an app like PillCaddy that everyone in the care circle uses, the structural requirement is the same: before giving a dose, you can see whether anyone else already did.
The coordination challenges in dementia caregiving are a more intense version of what any multi-caregiver family faces. If the care circle includes siblings or other family members dividing the daily work, coordinating medications across multiple caregivers covers the broader dynamics in depth.
A few coordination principles that help:
Designate a primary medication manager. Even with multiple caregivers, one person should own the overall medication plan: the current list, the schedule, the refill cadence, the communication with the doctor and pharmacist. Other caregivers can administer doses, but they're working from the primary's system, not improvising their own.
Document changes immediately. When a medication changes (new prescription, dose adjustment, discontinuation), update the shared record same-day. The most common source of dangerous errors is a caregiver giving a medication that was discontinued last week because they didn't know.
Have one source of truth for the schedule. Whether it's an app, a notebook, or a whiteboard, there should be one place that defines the current medication plan. Two notebooks with conflicting information is worse than one notebook with imperfect information.
Brief the new helpers. When a new caregiver joins (a new aide, a visiting relative), walk them through the medication system in detail before they handle any doses. Don't assume general competence translates into knowing your specific person's plan.
When professional help matters
A few situations are beyond what informal family caregiving can safely handle, and the right move is to bring in professional support rather than try to manage harder.
If the person is taking multiple complex medications with narrow therapeutic windows (blood thinners, insulin, anti-seizure medications, certain heart medications), the consequences of dosing errors are significant. A consultation with a pharmacist who specializes in geriatric medication management, or a referral to a medication therapy management (MTM) service, is worth the cost.
If the person is in advanced dementia and requires hands-on administration for every dose, but caregivers can't reliably be present at every dose time, in-home health aide support is the answer. Aides can be hired through home health agencies for partial-day or full-day coverage, often partially covered by long-term care insurance or Medicare (depending on the specific situation and benefits).
If medication management is one of several care needs that have become overwhelming, a geriatric care manager can assess the overall situation and coordinate services. The National Institute on Aging maintains directories and educational resources for finding professional caregiving support.
And if you're the primary caregiver and you're exhausted, the medication problem is often a symptom of a larger caregiver-stress problem. Respite care, adult day programs, and support groups exist for exactly this reason. Asking for help isn't a failure; it's how serious caregiving stays sustainable.
A closing word
If you've read this whole article, you're carrying something hard. Caring for someone with dementia is one of the most emotionally and logistically demanding situations adult life produces, and the medication management piece is just one part of a much larger picture.
A few things worth saying about that.
You won't get everything right, and that's okay. Doses will get missed. Routines will fall apart. You'll forget something at the worst possible moment. Your loved one will be confused or upset in ways that aren't your fault. Build a system that's resilient to imperfection rather than one that requires perfection.
The system you build today will need to evolve. Dementia progresses, and the strategies that work now will need to be revisited every few months. Build in the assumption that this is dynamic, not a one-time solution.
You don't have to do this alone. Whatever the other family dynamics are, medication management is one of the easier things to share if you have the right tools. PillCaddy is built for exactly this coordination problem: a shared household record where every family member with permission can see what was given and when, and add doses as they administer them. The free Essentials tier covers households up to two members, which is enough for a primary caregiver and the person being cared for. The Plus tier expands to more members for families with siblings, in-laws, or professional aides who are all part of the care circle.
Whatever combination of tools, family help, and professional support you end up with, the goal isn't a perfect system. It's a system that keeps your loved one safe while letting you sleep at night. That's enough. Some days it will feel like more than enough. Most days it will just be what you do. And that's the work.
A shared record everyone can check
PillCaddy gives the whole care circle real-time visibility into what was given, by whom, and when. Instead of asking whether your loved one took their pills, anyone can verify directly. Essentials is free; Plus covers families with multiple siblings, aides, and caregivers.
Frequently asked questions
How is managing medications for someone with dementia different?
Dementia breaks the normal loop where a person remembers taking a dose and can answer reliably when asked. Memory and self-reporting both become unreliable, and over time the person may stop recognizing their medications altogether. That makes outside verification and a consistent routine far more important than they would otherwise be.
Why shouldn't I just ask my parent whether they took their pills?
Someone with dementia may answer in good faith with information that does not match what actually happened, because the internal record keeping that supports an accurate answer is no longer working. Instead of asking, verify directly by checking the pill organizer, the blister pack, or a tracking record. This protects both their safety and their dignity.
What is the safest way to store medications for someone with dementia?
Many caregiver resources, including the Alzheimer's Association, recommend keeping medications in a locked drawer or cabinet to prevent accidental extra doses or a person taking medication that is not theirs. A single accessible weekly organizer that the caregiver refills can sit outside the locked store. Confirm any specific storage questions with your pharmacist.
My mom is starting to resist taking her medication. What can I do?
Resistance is common, and the underlying reason is not always clear. Rather than turning it into a confrontation, talk with the doctor or pharmacist about whether an alternative form or approach might fit. They can advise on options based on her specific situation.
How do my siblings and I keep track of who gave a dose?
The reliable answer is a shared record that everyone updates in real time and can check before giving anything. That can be a logbook on the counter or an app the whole care circle uses, as long as it is genuinely shared. PillCaddy is designed so anyone with permission can mark a dose as given and everyone else sees it immediately.
Do medication reminder apps work for someone with dementia?
Phone-based reminders can help in early-stage dementia when the person still uses their phone reliably, but they become less effective as the condition progresses and the person stops responding to prompts. At that point the value of an app shifts toward coordinating caregivers and recording what was given. No single tool solves dementia medication management on its own.
When should we bring in professional help for medication management?
Professional support is worth considering when the person takes high-risk medications, needs hands-on help for every dose that family cannot reliably provide, or when medication is one of several care needs that have become overwhelming. A pharmacist, a geriatric care manager, or an in-home aide can each fill a specific gap. Your loved one's care team can point you to the right resource.